

Quiana Bishop, DPC Board President
While dialysis treatments sustain life for people with kidney failure, they cannot replace all of the many functions of a healthy kidney. Patients rely on medications to address certain symptoms. As of January 1, 2025, all of these medications are included in the ESRD prospective payment system bundle and dialysis facilities are given the responsibility of dispensing them. This arrangement saves money for Medicare, but it does so by creating a profile for an “average patient” and discouraging expenditures on anyone else. As we know, there’s no such thing as an “average” patient, with the result that innovative treatments developed for those who need extra, are not getting to those patients who need them.
One of the conditions addressed by medications is phosphorus. Phosphorus is absorbed in the small intestines and stored in the bones. Healthy kidneys get rid of the extra amounts not needed in the body. Because unhealthy kidneys are no longer able to remove phosphorus from the blood and get rid of the excess in urine, high levels of phosphorus (hyperphosphatemia) is a problem for people with end stage renal disease.
This can cause bone and heart problems that lead to hospital stays and in some cases, death; calcification or hardening of tissues when phosphorus and calcium form deposits in the heart, arteries, joints, skin, or lungs that can be painful and lead to serious health problems; and puritis (itching).
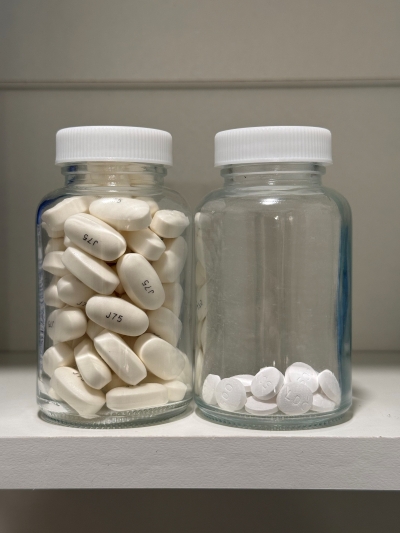
One week of typical phosphate binders (left) vs. one week of Unicycive’s new phosphate binders (right) pending approval later this year.
Until recently, the only treatment for high phosphorus was phosphate binders, large pills that must be taken in large quantities. Because I had a gastric sleeve done several years ago, the phosphorus binders expand in my now much smaller stomach. Then I can’t eat. If I can’t eat, I miss out on all the other nutrients and vitamins you gain from eating. So, I have battled with my phosphorus. I have tried all types of binders with not very good results. And all these years of uncontrolled phosphorus has caused calcium deposits throughout my veins, throughout my entire body, which complicates my eligibility for transplantation.
An innovative treatment for phosphorus is Xphosah, a phosphate blocker. I was prescribed and received this drug from my Medicare Part D plan until it was rolled into the ESRD bundle. It has worked well for me and I feel like if there was access to these new medicine years ago, I would be on the transplant list or, better yet, would have a kidney by now. But because of an impasse between the manufacturer, Ardelyx, and Medicare over the terms, Medicare no longer covers this drug. I am fortunate that Ardelyx is providing me with the drug for free for the time being, but this is not a sustainable solution for patients.
Ardelyx’s dispute with Medicare centers on whether its Transitional Drug Add-On Payment Adjustment (TDAPA) for new medications is inadequate. DPC thinks it’s not, and that new therapies need to be paid for separately in a sustainable manner.
There’s no guarantee that payment bundling will be safe and efficient for patients. First of all, it can’t be safe if there is significant variation in patients’ needs. The bundle intentionally incentivizes providers to administer less treatment. This can be helpful if excessive treatment is wasteful or dangerous. But when some patients require more than the standard treatment, providers may default to the usual care to avoid the extra expense.
For years, kidney care relied on old and inexpensive drugs to address various conditions. It did not matter that not every dialysis patient has ESRD-related puritis (itching) when the standard treatment was a Benadryl tablet that costs a penny. But the introduction of Korsuva, a drug to treat ESRD-related puritis, changed that. The requirement that this drug go in the bundle has resulted in a de facto embargo of the medication. Empirical research has found a prevalence of moderate to severe puritis among dialysis patients of 33 percent, but Korsuva has been dispensed to fewer than one percent of patients. CMS baked the artificially low take-up during the TDAPA period into the cake, adding a tiny amount to the bundle for the drug and locking in a depressed rate of utilization in perpetuity.
In my case, while most patients respond well to phosphate binders, I and many others do not. When the payment is fixed and Medicare treats me like the “average” patient, I become an expensive patient in the eye of providers. The experience under TDAPA is that we exceptional patients are not getting the new drugs.
Bundling also assumes that there are consensus protocols followed by clinicians when it includes dollars for a particular intervention. That is not always how things work, especially when an intervention is new. In the kidney care world, the management of dialysis organizations determines protocols and formularies for each of their clinics. If fewer than all providers implement a new drug in their facilities, and CMS averages the take-up across all patients, the new component of the payment will only partially reimburse the treatment for the adopting clinics, and leave a windfall for clinics sticking to the status quo. This scenario appears to be in play for two current TDAPA drugs that are not being adopted profession-wide.
Finally, bundling assumes that savings from new protocols benefit the provider. The bundled payment for hospitals incentivizes them to manage stays efficiently, and to drive a hard bargain with their suppliers. If they succeed, they keep the difference between the bundled price and their costs. Patients are protected by the right to a real-time appeal of discharges.
But the gains from new protocols in the ESRD bundle don’t go to providers. DefenCath is a catheter lock solution whose costs are borne by dialysis organizations while the benefits—reduced infections and hospitalizations—accrue mostly to patients and the Medicare Trust Fund. Vafseo, an oral HIF-PHI to treat anemia in dialysis patients, could reduce transfusions for patients who don’t respond to ESAs, but that too is a benefit to patients and to Medicare, not to the bundle gatekeeper. Meanwhile, patients can’t appeal a lack of access to a new therapy that their doctor hasn’t prescribed and that they most likely don’t even know about.
We now see drugmakers retreating from the development of dialysis drugs. Many millions of dollars were invested to improve kidney care, but manufacturers’ negative experience under bundling means venture capital is unlikely to make such investments in the future.
Fortunately for patients, kidney care champions in Congress have introduced legislation to remedy this problem. H.R. 6214, the Kidney Care Access Protection Act (KCAPA), would extend additional payments for innovative therapies. Visit https://kidneyaction.org/support-s-2730-hr-6214-the-kidney-care-access-protection-act/ or scan the QR code to contact your representatives in Washington and ask them to co-sponsor this important bill.


